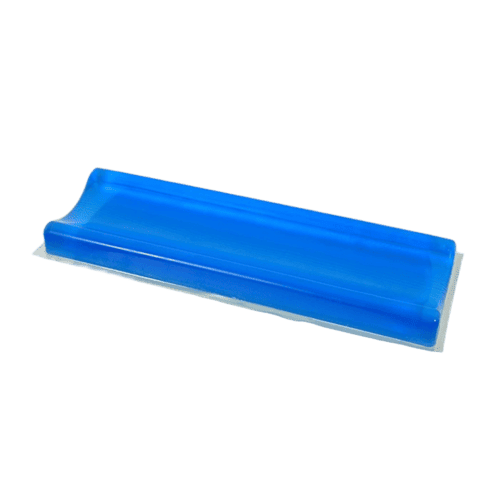
The AM-TW-012 solves a problem that sounds minor in a product catalog but becomes very real the first time you see a post-op patient with ulnar neuropathy because their arm was pressed against a flat table edge for three hours. The ulnar nerve runs superficially at the elbow — it’s the one that gives you the tingling when you hit your funny bone — and when a patient’s arm rests on a hard, flat surface for the duration of a prone spine case or a long lateral procedure, the nerve gets compressed between the bony medial epicondyle and the table. By the time the patient is extubated, they have numbness in the fourth and fifth fingers that can take weeks to resolve. That’s a positioning complication, not a surgical one, and it’s entirely preventable. The concave pad was designed so that limb contact force spreads across soft tissue instead of concentrating on a bony prominence.
At 50×15×4cm, the pad’s elongated geometry is deliberate. The concave trough runs the full 50cm length, which means you can position an entire forearm, a knee, or paired ankles along the channel without edge pressure at either end. The polymer gel formulation here is firmer than what we use in our head pads — I spec’d a higher durometer because limb positioning needs structural stability against the surgical field, not just cushioning. The pad needs to hold the limb in position when the surgeon leans in, not just make it comfortable. In prone knee cases, the trough keeps the patella suspended in the concave recess so the surgeon can access the popliteal fossa without the knee rolling laterally when pressure is applied. In lateral arm positioning, the channel prevents the dependent arm from sliding off the arm board when the table is tilted or when the surgical team leans against the drapes. The anti-slip base anchors to both the table and the arm board surface, and the gel’s viscoelastic response absorbs table adjustments without creating shear at the skin interface.
This pad is the workhorse of our non-head positioning line, but it serves a different purpose than our other limb supports. It doesn’t compete with the tunnel pad (AM-TW-014), which fully encircles the limb for 360-degree protection in lateral decubitus. It’s not the semi-circle (AM-TW-017), which is primarily a lateral torso and axillary support. The concave pad’s sweet spot is prone extremity positioning — knees, arms, ankles — where you need open surgical access above the supported limb and the limb needs to stay stable in a defined channel.