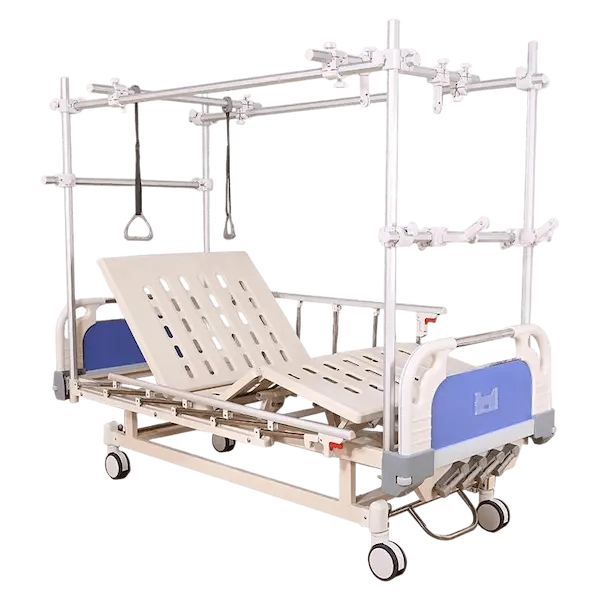
An orthopedic surgeon in Chengdu told me something I think about every time I look at the B01-III-16. “A femur fracture doesn’t heal in a bed that only moves the backrest. It heals when the leg is suspended at exactly the right angle, for exactly the right number of weeks, without the patient shifting position in their sleep and undoing three days of alignment progress.” General hospital beds treat the patient. Orthopedic beds treat the bone. The B01-III-16 is an orthopedic bed — four cranks, a traction frame, and the mechanical patience that bone healing demands.
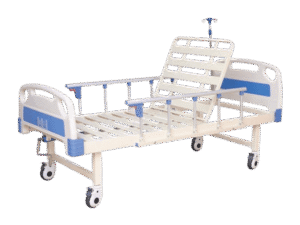
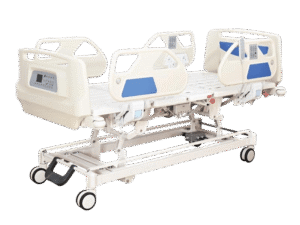
Four cranks means four independent adjustments. The backrest — same seventy-five-degree range as our two-crank beds, but here it’s just the starting point. The knee section — elevates the thigh and lower leg independently, creating the knee-break angle that offloads the sacrum and keeps the patient positioned in the bed rather than sliding down. The height adjustment — the entire mattress platform raises and lowers through a range of roughly fifty to seventy-five centimeters, which matters more for orthopedic patients than general ward patients because leg suspension requires precise height relative to the traction frame. And the Trendelenburg and reverse Trendelenburg tilt — the whole platform angles head-down or head-up by about twelve degrees, which for a trauma patient in shock is circulatory support; for a spine patient, it’s decompression.
The traction frame is the orthopedic-specific component. It’s a tubular steel overhead frame — sometimes called a Balkan frame — that mounts to the head and foot boards and provides anchor points for traction ropes, pulleys, and weights. The mounting points are reinforced steel brackets, not aftermarket clamps that work loose. A femur fracture in balanced suspension traction requires anywhere from five to fifteen percent of body weight hanging from precisely positioned pulleys over a period of six to twelve weeks. If the frame shifts, the traction vector shifts, and the bone heals at the wrong angle. The B01-III-16’s frame doesn’t shift.
The leg suspension bar attaches to the traction frame and supports the fractured limb in a Thomas splint or Pearson attachment — the standard rig for femoral shaft fractures. The bar adjusts longitudinally and vertically so the orthopedist sets the suspension angle during rounds and the nursing staff verifies it during checks. No tools required for adjustment — wing nuts and graduated markings, low-tech but unambiguous. The bed also accommodates cervical traction via a head-end pulley mount for cervical spine fractures, though that’s a less common application.
The mattress platform is perforated steel with ventilation that matters for a patient who’s immobilized for weeks. A bed-bound orthopedic patient is at high risk for pressure injury and respiratory complications, and both risks are amplified by a mattress that doesn’t breathe. The side rails are full-length aluminum, drop-down, with the two-step release mechanism. Casters are one hundred twenty-five millimeter twin-wheel with two locking. Weight capacity is one hundred seventy-five kilograms — de-rated slightly from our standard manual beds because the traction frame adds load complexity that requires conservative engineering.
The B01-III-16 is not a general ward bed. It’s heavier, more expensive, and more complex to set up than a two-crank manual. It belongs in orthopedic wards, trauma centers, and district hospitals that manage long-bone fractures surgically or conservatively and need a bed that holds a leg in traction for two months without drifting. If your ortho department has been making do with general ward beds and jury-rigged traction setups — pulleys tied to IV poles, weights balanced on chairs — the B01-III-16 replaces that improvisation with purpose-built engineering. Contact me.