I once visited a rural clinic in western Hunan that had twenty beds and a generator that failed twice a month during the rainy season. The clinic director showed me an electric bed someone had donated — it had been unplugged for a year because the power was too unreliable to depend on. “I don’t need a bed with a remote,” she said. “I need a bed that works when nothing else does.” That conversation is why I keep the AM-A01-III-01 in our line. It’s the simplest hospital bed we make — one crank, one function, no electricity required. And for a certain kind of facility, that’s not a compromise. That’s the point.
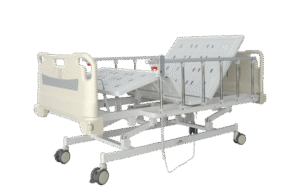
The A01-III-01 adjusts the backrest — and only the backrest. One crank at the foot of the bed, a worm-gear mechanism, and the head section rises from flat to about seventy-five degrees in a continuous sweep. That’s the one motion that matters most in a basic ward: sitting a patient up to eat, to breathe, to receive a respiratory exam. If you need knee elevation or height adjustment, those require two or four cranks, and that’s the A01-III-06 or the B01-III-16. But if your clinical need stops at “patient needs to sit up without a pile of pillows falling behind them every fifteen minutes,” one crank is enough.
The frame is powder-coated steel — rectangular tubing, welded joints, a finish that’s been salt-spray tested to two hundred hours. It’s not stainless steel, and I’m not going to pretend it is. But for a dry ward in a clinic or a rural hospital that sees normal humidity, it won’t rust through in any timeframe that matters. The head and foot boards are blow-molded ABS — plastic, not wood or laminate — which means they wipe clean with hospital-grade disinfectant and don’t delaminate at the edges like MDF boards do after a hundred cleanings.
The mattress platform is perforated steel sheet — four panels, the head panel hinged to the crank mechanism. Perforations let air circulate under the mattress, reducing the trapped moisture that contributes to pressure injury risk. The side rails are aluminum alloy, collapsible — push the release button and they drop below mattress level for patient transfer. They lock in the raised position with a spring detent that doesn’t work loose over time the way friction-fit rails eventually do.
The bed rolls on four casters — one hundred twenty-five millimeter diameter, two of them locking. The casters are the same twin-wheel design we use on our electric beds because I’m not going to downgrade the rolling hardware on a manual bed. A nurse pushing a bed down a corridor shouldn’t feel a quality difference just because the bed cost less. The weight capacity is one hundred seventy-five kilograms — conservative, because a bed that gets used by rotating patients in a ward will occasionally see someone heavier than the average.
Who buys the A01-III-01? Rural clinics where the power supply is uncertain and maintenance staff is one person. Field hospitals and temporary medical facilities where simplicity equals reliability. Small nursing homes where backrest positioning is the only clinical positioning the staff actually uses. If you need knee elevation, step up to a two-crank model. If you need full positioning, go electric. But if you need a bed that adjusts the backrest, rolls when pushed, and doesn’t care whether the generator is working — the A01-III-01 is the bed that clinic director in Hunan should have had from day one. Send me your ward description and I’ll tell you whether one crank covers it.