The first time I saw a patient monitor fail, I was a junior product manager shadowing an ICU nurse on a night shift. The monitor — a brand-name unit, five years old — started throwing artifact on the ECG lead and alarming on what turned out to be nothing. The nurse silenced it without looking up. She’d been working with that unit long enough to know its quirks, and she trusted her own assessment over the machine’s crying wolf. That’s the difference between a monitor that earns its place in a clinical workflow and one that just takes up a mounting arm: reliability you don’t have to think about.
The AM-SNP900N is our standard multi-parameter patient monitor — five parameters, one box, and I mean “standard” the way clinicians mean it. Not stripped-down. Not overloaded with features nobody asked for. It measures ECG, SpO2, non-invasive blood pressure, temperature, and respiration. That’s the set of vitals that covers about ninety percent of continuous monitoring situations in an emergency department, ICU bay, post-anesthesia care unit, or ambulance transport. You can add ETCO2 via an optional module if your protocols call for it. But the core five are what most departments actually use, and we optimized for those.
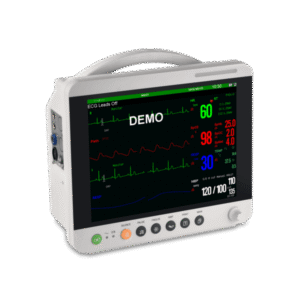
The display is a twelve-inch TFT color LCD at 800 by 600 resolution. Not the highest pixel density on the market, but absolutely readable at arm’s length from a nurse’s station — and more importantly, glanceable. Waveforms are smooth, numerics are large, and alarm thresholds are color-coded: yellow for warning, red for critical. I’ve watched nurses scan a bank of monitors in under two seconds during rounds, and that speed is a function of layout clarity, not screen specs. The trend storage holds seventy-two hours of data at one-second resolution, which covers most post-op observation windows and gives the attending physician a honest picture of what happened overnight.
The fanless design matters more than the spec sheet suggests. A quiet monitor is a non-negotiable in recovery wards and NICUs where ambient noise directly affects patient outcomes. It also means the internal electronics aren’t actively pulling dust and lint through the chassis, which extends the service life in environments that aren’t exactly cleanrooms. The housing is rated IPX1 — protected against vertically falling water drops, so an IV bag leak or a splash during cleanup won’t kill the unit. If somebody spills a full basin of water on it, that’s a different conversation, but the day-to-day liquid exposure of clinical work is managed.
Connectivity is wired — Ethernet jack on the back for central monitoring station integration — plus standard nurse-call relay output. No wireless module, which keeps the regulatory path shorter and the price lower. If your facility runs a centralized monitoring system, the SNP900N drops in with standard HL7 output. If you’re using it standalone in an ambulance, the internal battery runs about four hours on a full charge, which covers most inter-facility transfers with margin.
I’m not going to pretend this monitor competes with a Philips or GE high-end unit on features. It doesn’t do invasive pressure monitoring, cardiac output, or BIS. What it does is cover the five parameters that every acute care setting needs, on a platform that doesn’t crash, doesn’t overheat, and doesn’t produce so many nuisance alarms that nurses learn to ignore it. For ER bays, recovery rooms, rural hospital ICUs, and ambulance fleets that need volume — put the same monitor in every bay and your clinical staff only has to learn one interface — the SNP900N is the workhorse. Drop me a line with your bed count and I’ll put together a package that makes sense.