7 Critical Factors for Choosing Surgical Pendants: The 2026 Hospital Buyer’s Guide
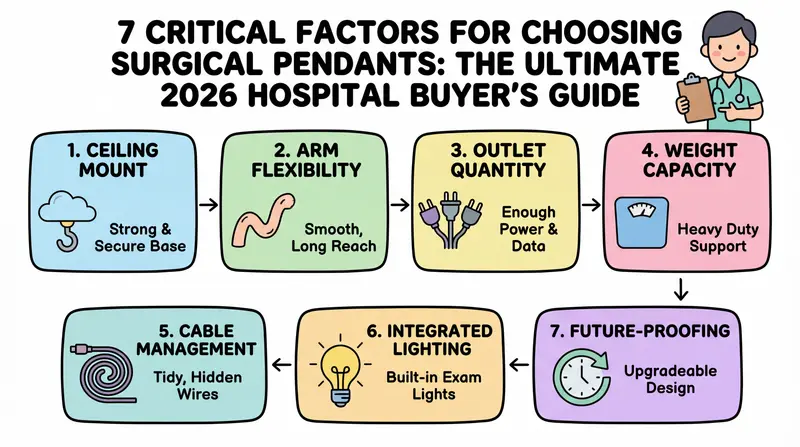
7 Critical Factors for Choosing Surgical Pendants: The Ultimate 2026 Hospital Buyer’s Guide
A surgical pendant is not “just a ceiling boom.” It is a safety system, a workflow tool, and a long-term cost decision. This guide covers types, configurations, drive systems, standards, installation, and procurement FAQs â so your next OR upgrade improves outcomes, not just aesthetics.
The first time I walked into a newly renovated operating room, everything looked perfect. Bright ceiling. Clean walls. Quiet machines.
And then the case started.
A monitor arm drifted a few centimeters. A cable loop touched the floor. Someone stepped back, and the anesthesia line pulled tight for a second.
No one panicked. But everyone felt it. That tiny “almost” moment.
Many OR safety incidents are not caused by people. They are caused by infrastructure that forces people to improvise.
A ceiling-mounted pendant system is not a luxury accessory. It is the difference between an OR that behaves predictably, and an OR that constantly surprises you.
| Feature | Electric Surgical Pendant | Mechanical / Manual Pendant |
| — | — | — |
| Arm Configuration | Single Arm / Double Arm | Fixed or Manual Swivel |
| Brake System | Pneumatic or Electromagnetic | Mechanical Friction Brake |
| Load Capacity | Heavy-duty (up to 300 kg) | Standard (up to 150 kg) |
| Rotation Angle | 330° â 340° Horizontal | 330° Horizontal |
| Material | High-strength Aluminum Alloy | Medical Grade Stainless Steel |
| Applications | ICU, Anesthesia, Surgery | Endoscopy, Minor Procedures |
Most procurement discussions start with a checklist: how many shelves, how many sockets, what is the load capacity. Those matter. But they are not the real decision.
The real decision is: what kind of behavior do you want your operating room to enforce every single day?
Because the pendant is the “organizing system” of gas outlets, power, data, monitors, and devices. When it is chosen well, it reduces clutter and improves operating room efficiency. When it is chosen poorly, it becomes an expensive bottleneck hanging from the ceiling.
—
The Evolution of Modern OR Infrastructure
A decade ago, many ORs relied on carts, floor stands, and long cable runs. It worked, until it did not.
More devices entered the room. More screens. More documentation. More energy demand. The floor became crowded. The “clean” zone and “busy” zone blurred.
That is why the pendant system became central to modern OR design. It is not only about looking tidy. It is about removing friction from clinical work: fewer obstacles, fewer trip hazards, and faster repositioning.
The most advanced OR is not the one with the most devices. It is the one with the least chaos.
—
Classification by Clinical Function
Not all pendants are built for the same mission. If you buy one “general” solution for every room, you often end up with compromises everywhere.
1) Anesthesia Pendants
An anesthesia pendant is built around gas management and stable equipment placement. It typically supports the anesthesia machine workflow, vaporizer access, and integrated gas outlets.
The key is not the number of outlets alone. It is how safely and consistently the clinical team can connect, disconnect, and verify lines under pressure.
2) Endoscopy and Surgery Pendants
Endoscopy and surgical configurations often prioritize display positioning, instrument integration, and quick repositioning. Monitors must move smoothly, stay stable, and lock reliably.
In minimally invasive surgery, “screen position” is not comfort â it is performance. A few degrees of mismatch can mean longer cases and more fatigue. When pairing a pendant with surgical lights equipped with integrated 4K cameras, monitor positioning becomes even more critical.
3) ICU Bridge Pendants
ICU bridge pendants are often used in critical care environments where bed access and organized supply matter. They support oxygen, power, and data distribution while keeping floor space usable.
Different department, same principle: predictable access without crowding.
Choosing the wrong pendant type is how hospitals accidentally pay for features they cannot use â and miss the ones they need daily.
—
Configuration: Single Arm vs. Double Arm
This is where many projects look simple on paper and messy in the room.
A single arm pendant can be the right choice when:
- The room has a stable layout.
- The equipment set is relatively fixed.
- You want fewer moving joints and a simpler footprint.
A double arm pendant shines when:
- You need flexible coverage across multiple working positions.
- Different specialties use the same OR.
- You need to reach the patient zone without dragging cables or carts.
But do not treat “more arms” as automatically better. More joints mean more complexity. What you really want is the right movement envelope for your clinical reality.
What to Check Beyond Load Capacity
Load capacity should be evaluated honestly, not optimistically. Ask what will be mounted in year one and what will be added by year three. Hospitals rarely remove devices â they add them.
Also check:
- How the load is distributed across shelves and rails.
- Whether the arm remains stable when fully extended.
- How easy it is to reposition without drift.
The best pendant is not the one that can carry the most. It is the one that can carry your real setup without fighting you.
—
Drive Systems: Electric vs. Manual
This is a classic procurement debate. And the truth is: both can be correct. It depends on how your team works and how your hospital maintains assets.
Electric Surgical Pendant
Electric height adjustment can improve ergonomics and reduce repetitive strain. It can also support faster room turnover when different teams need different working heights. But it introduces electrical and control components that must be maintained properly.
The question is not “Is electric premium?” The question is “Can we sustain the maintenance discipline that electric systems deserve?”
Manual Medical Pendant
Manual systems are simple and often more forgiving in environments with limited maintenance bandwidth. A well-designed manual pendant should still move smoothly and lock reliably.
Do not accept “manual” as an excuse for rough motion or unstable positioning. If repositioning feels difficult, staff will stop adjusting it. And then your “flexible” system becomes static.
Technology does not create efficiency. Adoption creates efficiency.
—
Technical Specifications and Safety Standards
This is where you build real buyer confidence and long-term risk control. Because pendants are not just mechanical arms â they are medical electrical systems, gas distribution interfaces, and movement systems operating above a patient.
Standards and Compliance Mindset
Look for a supplier that can speak clearly about:
- IEC 60601-2-41 (where applicable to relevant equipment context)
- Electromagnetic Compatibility
- Gas outlet safety and verification processes
Even if your local regulation differs, a supplier’s ability to discuss testing logic matters. It shows maturity.
Braking and Stability
In daily use, braking is everything. A pendant that does not lock confidently creates micro-stress all day.
Ask directly about braking design:
- Mechanical braking principles
- Pneumatic braking options (if available)
- How the system behaves under full load and full extension
And then ask the most practical question: what happens after two years of daily use? If the answer is vague, that is a signal.
In the OR, “almost stable” is not stable. Reference: WHO Medical Device Technical Series.
—
The Hidden Cost of Wrong Decisions
Most hospitals evaluate pendants like furniture. But the OR team experiences pendants like a safety instrument.
When the pendant design is wrong, the team compensates with habits:
- Leaving cables longer “just in case.”
- Avoiding repositioning because it is annoying.
- Parking carts in the wrong zone because the boom cannot reach.
And suddenly your new OR is not more efficient. It is just more expensive.
A poor pendant forces workarounds. And workarounds are where risk hides.
The best ROI does not come from buying the highest configuration. It comes from eliminating the everyday friction that steals minutes, focus, and confidence from every case.
—
Installation and Maintenance Guide
A ceiling-mounted pendant is only as good as the infrastructure supporting it. If installation is treated as “just mounting,” you will pay for it later.
Installation: What Must Be Clarified Early
Before purchase, align on:
- Ceiling structural capacity and reinforcement plan
- Mounting points and room layout coordination
- Pathways for gases, power, and data
- Service access for future maintenance
This is part of operating theatre infrastructure planning, not a last-minute detail. Also clarify who owns which scope: hospital, contractor, or supplier. When responsibilities are unclear, schedules slip and quality suffers.
Maintenance Reality Check
Ask for a practical maintenance plan:
- Inspection intervals
- Wear parts and expected lifecycle
- Response time and spare parts availability
- Documentation and training
If your team cannot maintain what you buy, you do not own the pendant. You rent downtime in advance.
The cheapest pendant is the one that does not interrupt surgery.
—
Evidence & Market Data
- Market size: Global surgical pendant market valued at $540 million (2025), growing at 5.4% CAGR to 2030 (MarketsandMarkets).
- Regulatory standards: IEC 60601-1 governs medical electrical equipment safety; ISO 11197 specifies requirements for medical supply units including surgical pendants.
- Load capacity: Standard ceiling-mounted pendants rated 150–400 kg total load; individual monitor arms support 20–40 kg each.
- Gas terminal durability: O₂, medical air, N₂O, vacuum, and AGSS terminals are tested to 10,000+ connect/disconnect cycles under ISO 11197 compliance.
- Installation timeline: A typical OR pendant installation requires 2–3 days, including ceiling structural reinforcement and medical gas line connection.
- Cost range: A dual-arm ceiling surgical pendant system typically costs $12,000–$35,000 depending on arm configuration, gas terminal count, and accessory loadout.
Frequently Asked Questions
What is the best material for surgical pendants?
Many modern systems use aluminum alloy due to its balance of strength, weight, and corrosion resistance. But focus on engineering quality, not only material name. Ask about surface treatment, cleaning compatibility, and long-term durability under disinfectants.
How many gas outlets should an anesthesia pendant have?
It depends on your anesthesia workflow, local standards, and case mix. Start by mapping your typical setup and your peak setup, then plan for realistic expansion. A better question is: how will you prevent misconnection and manage line organization under pressure? Safety is not only quantity â it is clarity.
Can I customize the number of power sockets?
In most projects, yes â within safety and design constraints. When customizing, ensure clear labeling and logical grouping, protection against overload, considerations for electromagnetic compatibility, and access that does not force cables to cross walking paths. Customization is valuable only when it improves behavior, not when it creates complexity.
Shoule I choose a ceiling-mounted or wall-mounted pendant?
Ceiling-mounted pendants offer the most flexibility for OR workflow because they provide 330°+ rotation and can be positioned anywhere above the surgical field. Wall-mounted options work better in smaller rooms or recovery areas where ceiling structural support is limited. Always verify ceiling load capacity before committing to a ceiling mount.
—
Final Thoughts: Choose by Function, Not by Spec Sheet
A surgical pendant is not a line item. It is a daily system that shapes safety, speed, and consistency.
Choose by clinical function. Confirm movement coverage. Be honest about load capacity. Decide electric vs. manual based on adoption and maintenance reality. And treat installation as part of infrastructure, not decoration.
When planning your OR upgrade, consider how the pendant integrates with your LED surgical lights and other operating room equipment â because in a real operating room, the floor, the ceiling, and the workflow are always connected.