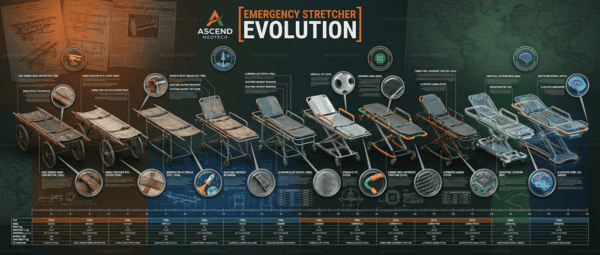
The Evolution of the Emergency Stretcher: From Battlefield Improvisation to Advanced Life Support Platforms ascend medtech
The Evolution of the Emergency Stretcher: From Battlefield Improvisation to Advanced Life Support Platforms ascend medtech
Prepared by: Emergency Medical Equipment Specialist Subject: Historical Analysis of Patient Transport Devices (PTDs)
1. Introduction
The emergency stretcher, historically referred to as a “litter,” constitutes the fundamental interface between the pre-hospital environment and definitive care. Its evolution parallels the advancement of paramedicine, shifting from a passive device for simple evacuation to a sophisticated, ergonomic platform designed for Advanced Life Support (ALS) and the prevention of Musculoskeletal Disorders (MSDs) in healthcare providers.
2. Historical Epochs and Technological Milestones
Era I: Pre-20th Century — The Era of Improvisation and Manual Carry
In antiquity and medieval times, transport was rudimentary. The primary objective was rapid evacuation from battlefields, often with little regard for spinal integrity or patient comfort.
- Ancient Context: Early designs utilized wicker, wood, or simple canvas suspended between two poles.
- Late 19th Century (The Industrial Shift): The necessity of the American Civil War (1861–1865) and the Crimean War drove the first standardization.
- The “Furley” Stretcher (1880s): Developed by Sir John Furley, this marked one of the first mass-produced “standard army patterns” featuring telescopic handles and canvas beds.
Era II: Early 20th Century — Standardization and Field Utility
During WWI and WWII, the focus remained on lightweight, stackable designs for mass casualty incidents (MCI).
- The Pole Stretcher: The ubiquitous canvas-and-pole design became the NATO standard. While effective for carrying, it offered no spinal support and required two to four bearers.
- The Stokes Basket (1904): Invented by Charles Francis Stokes. This wire-mesh basket revolutionized maritime and vertical rescue, allowing for the secure immobilization of patients during difficult extrications. It remains the progenitor of modern Search and Rescue (SAR) basket litters.
Era III: Mid-20th Century — The Rise of the Ambulance Cot
With the advent of civilian ambulance services in the post-WWII era, the requirement shifted from “carrying” to “rolling.”
- 1950s – Introduction of the Wheeled Cot: The integration of wheels and an undercarriage allowed for single-operator movement on flat surfaces.
- The X-Frame Design: This became the industry standard for decades. It allowed the cot to be raised for patient care and lowered for loading into the ambulance. However, it required significant manual lifting force (dead-lifting) by EMS personnel.
Era IV: Late 20th Century — Spinal Immobilization and Ergonomics
The 1970s and 80s saw a paradigm shift in trauma care, specifically regarding Pre-hospital Trauma Life Support (PHTLS) principles.
- The Scoop Stretcher (Orthopaedic Stretcher): Invented to split vertically into two halves, allowing EMS providers to “scoop” a patient without rolling them, minimizing spinal movement in pelvic or femur fracture cases.
- The Long Spine Board (LSB): While now used restrictively due to pressure ulcer risks, the LSB became the gold standard for full-body immobilization during this era, often used in conjunction with the stretcher.
- The H-Frame and Multi-Level Cots: Manufacturers like Ferno and Stryker introduced cots with multiple height positions to facilitate patient transfer from hospital beds.
Era V: 21st Century — Power-Load Systems and Bariatrics
The modern era focuses on two critical factors: Provider Safety (reducing back injuries) and Bariatric capabilities (managing obese patients).
- Powered Ambulance Cots (Early 2000s): The introduction of electro-hydraulic systems (e.g., Stryker Power-PRO). These utilize battery-operated hydraulics to lift the patient, effectively eliminating the manual lift for paramedics.
- Automatic Loading Systems: Tracks installed in the ambulance floor that physically lift the cot into the vehicle.
- Negative Pressure Isolation: Following the SARS (2003) and COVID-19 pandemics, stretchers began integrating with “Iso-Chambers”—portable negative pressure units for biohazard containment.
3. Key Timeline of Innovations ascend medtech
| Era / Year | Innovation / Event | Clinical Significance |
|---|---|---|
| c. 1380 | First documented “Litter” | Simple wicker/wood frame; limited clinical utility beyond movement. |
| 1861 | Civil War Standardization | Mass production of uniform litters for triage and train transport. |
| 1904 | Stokes Basket Patent | Revolutionized vertical and maritime extraction; focused on patient envelopment. |
| 1950s | The Wheeled Ambulance Cot | Transition from “bearers” to “operators”; facilitated care during transport. |
| 1970s | The Scoop Stretcher | Addressed the need for atraumatic lifting (minimizing patient manipulation). |
| 1994 | EN 1789 Standard (Europe) | Set rigorous crash-test standards (10g force) for stretcher retention systems in ambulances. |
| 2004 | Electro-Hydraulic Cots | The pivot point for EMS safety; drastically reduced lumbar strain and workers’ comp claims. |
| 2014 | Bariatric Power-Loaders | Systems capable of lifting 700+ lbs (318+ kg), addressing the obesity epidemic. |
4. Current State of the Art: The Modern Platform ascend medtech
Today’s “stretcher” is more accurately described as a Mobile Patient Management Platform. Key features include:
- Independent Leg Operation: Allows for loading into ambulances with high floors or uneven terrain.
- Retractable Head/Foot Sections: For maneuverability in tight urban elevators or stairwells.
- Integrated IV Poles and O2 Storage: Self-contained critical care setups.
- Knee-Gatch Positioning: Elevating the legs to treat shock (Trendelenburg position) or abdominal pain (Semi-Fowler’s position) comfortably.
5. Conclusion
The trajectory of emergency stretcher development has moved from a philosophy of expedience to one of clinical excellence and safety. The modern device protects the patient from secondary injury (spinal handling) and the provider from occupational hazards (lifting strain), serving as the foundation of pre-hospital care.