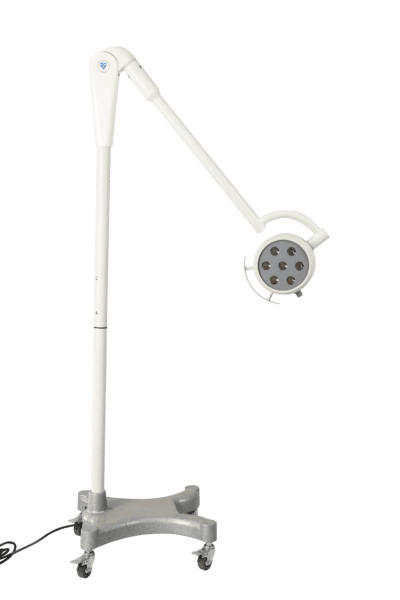
A physical therapist I work with runs her practice out of a converted retail space — eleven-foot ceilings, narrow treatment bays, and exactly zero extra floor area. When she asked me what exam light she should buy, I didn’t pitch her the mobile version. She had no place to park it. What she needed was a light that lived overhead and stayed out of the way until she reached up and pulled it down. That’s the AM-LED200-2 — same core technology as the floor-standing model, but fixed-mount, higher output, and designed for rooms where the floor already belongs to treatment tables, supply carts, and the people doing the work.
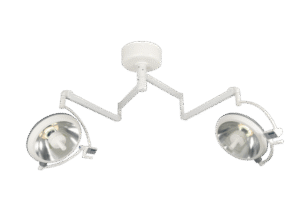
The AM-LED200-2 is the mounted configuration of our examination light platform, available in both ceiling-mount and wall-mount versions. If you have the ceiling height and want maximum positioning range, go ceiling. If your ceiling is too high, obstructed by ductwork, or you simply prefer the light at arm level, wall-mount puts the articulating arm right where you need it. Either way, the head articulates through a wide range of motion — pull it down for the exam, push it away when you’re done, and it stays put. The arm assembly uses spring-balanced joints that hold position without locking knobs. One-handed operation matters when your other hand is holding a speculum or dermatoscope.
We boosted the output to approximately 30,000 lux at one meter — a meaningful step up from the 20,000-lux floor model. That extra intensity helps in rooms where ambient light levels are already high, like procedure suites with large windows or open clinic bays with overhead fluorescent panels. It also makes a difference for deeper cavity exams: when you’re looking into an ear canal, nasal passage, or the posterior pharynx, extra lux translates to better visualization of mucosal surfaces and subtle color changes. The LED array is the same long-life platform — 50,000-plus hours rated, CRI above 90, 4,500K color temperature. No heat buildup that makes patients flinch.
The mounting plate works with standard North American junction boxes — a 4-inch octagonal ceiling box or a rectangular wall box at the right height, and the bracket mates directly. Electrical connection is line, neutral, ground. Any licensed electrician can install in under an hour, and we include a drilling template in the box. The arm assembly then clips onto the mounted bracket — no scaffolding, no specialty tools. Set screws come pre-applied with thread locker so foot traffic vibration doesn’t loosen anything over years of daily use.
The real advantage of a mounted light is workflow predictability. In a busy outpatient clinic — dermatology, ENT, wound care, sports medicine — the clinician knows exactly where the light is every time. No hunting for it because someone borrowed it for room 4. No wrestling casters over door thresholds or extension cord trip hazards. The light is part of the room, like the sink or the exam table. When you’re seeing thirty patients in a day, shaving ten seconds off every lighting adjustment adds up. Not to mention the reduced physical strain of not bending down to reposition a floor stand.
This light fits best in established practices where exam rooms have permanent layouts: private dermatology offices with dedicated procedure rooms, ENT clinics where every bay needs its own illumination, physical therapy facilities that want hands-free positioning for range-of-motion assessments, and teaching clinics where multiple students need to observe the same field. It’s also a smart choice for clinics subject to accreditation standards that want permanently installed, inspection-ready fixtures.
If you’re deciding between the floor-standing model and this one, the question is simple: do your exam rooms move, or do they stay put? If they stay put, mount the light and reclaim your floor. Drop me a line for ceiling height requirements, wall-mount arm reach specs, or lux distribution comparisons between the two configurations. I read every inquiry personally.